
Campinas has a Human Development Index (HDI) considered very high (0.805) and an urbanization rate of 98.28%, figures often comparable to those of high-income countries. However, a detailed epidemiological survey conducted by researchers from the Center for Theranostic Innovation in Cancer (CancerThera), based at the Hematology and Hemotherapy Center of the State University of Campinas (Hemocentro/Unicamp), reveals a concerning reality: social vulnerability in the municipality is a determining factor for cancer mortality.
Currently, according to the latest demographic census, Campinas is home to more than 1.186 million inhabitants. Using data from the Population-Based Cancer Registry (PBCR) of Campinas — one of the few in the country audited and certified by the International Agency for Research on Cancer (IARC), an entity linked to the World Health Organization (WHO) — researchers mapped disparities in diagnosis and lethality of the most common tumors among residents: prostate, stomach, breast, lung, oral cavity, cervical, and colorectal cancers.
The study analyzed consolidated data from 10 consecutive years (2010 to 2019), crossing information from the PBCR with the Mortality Information System (SIM) of the Federal Government and the São Paulo Social Vulnerability Index (IPVS), maintained by the State Government, to assess cancer incidence and mortality, shedding light on how the disease unequally affects rich and poor populations within the same municipality.
For statistical purposes, the Relative Index of Inequality (RII) was used, which quantifies the magnitude of health inequalities by ordering social strata from lower to higher socioeconomic vulnerability based on the cumulative population distribution. In the study, the RII was applied to evaluate disparities in cancer incidence and mortality across different cancer types in Campinas over two time periods (2010–2014 and 2015–2019). In addition to measuring inequality in each period separately, researchers used the RII linked to a temporal interaction term to assess whether inequity in access to cancer diagnosis and treatment worsened, decreased, or remained stable over the analyzed decade.
Dr. Carmino Antonio de Souza, onco-hematologist physician, professor at the School of Medical Sciences of Unicamp, and principal investigator of CancerThera, highlights one of the main paradoxes revealed by the study. “The city as a whole is powerful, with one of the highest HDIs in Brazil, but it is not homogeneous. You have areas with ideal HDI, comparable to Scandinavian countries, for example, but there are regions with numerous vulnerabilities,” evaluates the researcher, who also served as Campinas Health Secretary from 2013 to 2020.
The article resulting from the study has just been published in the scientific journal Cancer Epidemiology (volume 103) under the title “The impact of social inequalities on cancer incidence and mortality in a Brazilian city: data from the Population-Based Cancer Registry.”
Differences among cancer types and population inequalities
When applying the lens of socioeconomic inequality, the study found drastic and even increasing differences. One of the most paradoxical findings is that the overall incidence of cancer (the sum of all diagnoses) is statistically lower among the most vulnerable populations. However, overall mortality is significantly higher in these same groups. According to the researchers, this demonstrates a serious problem of underdiagnosis: poorer people are not getting sick less often; they simply do not have access to tests to detect the disease, which explains why they die more and faster when they finally reach the healthcare system.
In the case of prostate cancer, although incidence (new cases) modestly declined among the male population of Campinas, mortality inequality increased significantly: the risk of death became three times higher among the most vulnerable (poorest) men in the period from 2015 to 2019 when compared to the previous five years. Some explanations lie in sociocultural barriers such as lower educational levels, lower health literacy, and prejudices related to digital rectal examination, which contribute to delayed healthcare seeking, usually only when symptoms are already severe.
Dr. Andrea Paula Bruno von Zuben, epidemiologist and associated researcher at CancerThera, reinforces that this fact is due to profound structural variations. “Men in situations of greater vulnerability depend almost exclusively on the Brazilian Unified Health System (SUS), where they face longer waiting times for specialized consultations, diagnostic exams such as Prostate-Specific Antigen (PSA), biopsy and MRI, and for the beginning of treatment,” she explains.
She adds: “As a consequence, a large proportion of these patients receive diagnosis at more advanced stages of the disease, which reduces the chances of cure and clinical control.” Men with lower social vulnerability, on the other hand, have faster access to urologists, undergo earlier diagnosis, and begin treatment in a timely manner, substantially increasing survival chances.
Another relevant finding concerns oral cavity cancer, whose mortality inequality also remained consistently higher, with the risk of death reaching 3.3 times higher among the poorest populations. According to Zuben, failures in local primary care may be influencing the problem. “The proportion of oral health teams within SUS is below ideal for the population size, with focus still heavily centered on curative procedures, such as restorations and extractions, to the detriment of systematic screening and active search actions,” warns the researcher, also emphasizing that simple mouth lesions may evolve into fatal cases due to delayed access to biopsies and head and neck surgeries.
Regarding stomach cancer, although Campinas follows the national trend of overall decline in incidence and mortality among men, the study reveals that the disease still affects poorer populations more intensely. Data show that socially vulnerable men continue to present the highest rates of illness and death due to barriers in access to early diagnosis and greater exposure to risk factors such as genetic factors, excessive salt consumption, foods stored outside refrigeration, and finally the Helicobacter pylori bacterium, associated with several types of gastric tumors.
The scenario is worse among women, who experienced the emergence of a new disparity: while at the beginning of the previous decade incidence affected different social groups similarly (without inequality), between 2015 and 2019 stomach cancer began to affect low-income women more intensely. For researchers, the worsening of this disparity highlights the urgent need for public health policies focused on equity to ensure that the general decline in numbers does not mask disease progression in peripheral areas.
The CancerThera study also elucidates overall averages when analyzing women’s health, revealing an abyss between social classes. Breast cancer, for example, presents higher incidence among less vulnerable women (the wealthiest), but this is a consequence of reproductive factors (such as having children later or not having children, as well as fewer pregnancies) and greater access to preventive exams (such as mammography and ultrasound). Mortality also follows this group due to the high incidence of the disease; however, rapid access to healthcare networks allows higher cure rates, unlike women in vulnerable areas, who frequently discover the disease at advanced stages.
At the other extreme, cervical cancer — a highly preventable disease through vaccination against Human Papillomavirus (HPV) — has almost disappeared as a cause of death in wealthy areas of Campinas, but remains significant in the municipality’s more vulnerable regions, where it is 3.6 times higher. “When you observe cervical cancer in the city as a whole, it disappears from the top 10 causes of cancer death, but when you go to a more vulnerable region, it is still present,” exemplifies the researcher.
Another important warning for public managers brought by the study is the increase in incidence and mortality from lung cancer among women. Unlike what occurred in the past, deaths of women from lung tumors showed a strong upward trend, reflecting delayed consequences of changing habits, such as increased smoking among women. “This pattern is consistent with what worldwide epidemiological literature documents regarding the gender transition in smoking,” evaluates Andrea von Zuben.
The researcher says that although Campinas has important resources and initiatives to address lung cancer, the city faces structural challenges such as pressure on the public healthcare network: “Recent reports demonstrate increased oncology care demand and waiting lists to begin treatment, highlighting the need for more installed capacity and agility in diagnosis and treatment, especially for vulnerable groups.”
Colorectal cancer (or bowel cancer) faces difficulties related to offering complex exams such as colonoscopy on a large scale within SUS. The study identified a transition period: inequality in incidence of this disease, which was previously much more common among wealthier populations, is decreasing among different social classes in the city. However, a concerning finding was registered among men: overall mortality from the disease increased and inequality underwent inversion, indicating that deaths from bowel cancer are beginning to concentrate among the most vulnerable male population. Colorectal cancer, strongly associated with consumption of ultra-processed foods, obesity, and sedentary lifestyle, may become one of the leading causes of preventable death among poorer populations in coming years.
Deep research to support public policies
The national situation of diagnoses at advanced stages is still seen as a bottleneck. “It is embarrassing. We have a volume of advanced case diagnoses that is not compatible with the level of development we have. And then, of course, if diagnosis is late, prognosis is worse,” laments Carmino de Souza, reinforcing that robust local data are the main tool to reverse this context.
Since 2017, a municipal law (Law No. 15,371/2017) has made cancer a compulsory notification disease in Campinas. Today, a technical team from the Municipal Health Department actively monitors dozens of pathology laboratories, ensuring that no diagnosis goes unnoticed, regardless of whether the patient is treated within SUS or the private network.
The objective of the study authors, by disseminating and interpreting PBCR, SIM, and IPVS data, is to support local and state public health management in confronting inequities. For them, the systematic use of geographic and high-quality information is the main strategy to direct screening, strengthen primary care, anticipate diagnoses, and effectively save lives through adequate treatment.
Historically, the Campinas PBCR itself has already served to alter screening policies in the city: after noticing a high rate of aggressive breast cancer cases among younger women, the municipality anticipated the age for mammography before federal recommendation. “Public policy in cancer is not about reducing the number of cases, because it will not decrease. Public policy is about making more and more diagnoses and trying to prevent disease progression,” argues the researcher.
LEARN MORE
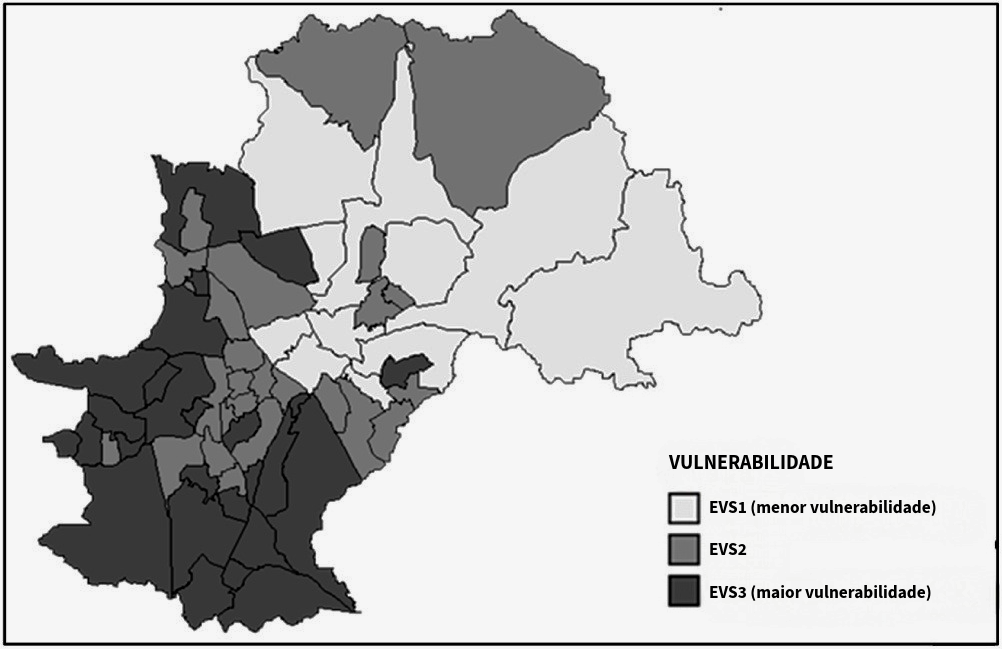
To understand inequalities, researchers did not analyze the city as a single block; they used the service map of all UBS units in the municipality and calculated a social “score” for each one based on socioeconomic data from the State of São Paulo. The map above summarizes this data crossing by dividing the territory into three major zones: SVS1 (Light Areas) – Neighborhoods and regions with the lowest social vulnerability (wealthier populations); SVS2 (Intermediate Areas) – Transition regions; SVS3 (Dark Areas) – Peripheral regions with the highest social vulnerability (poorer populations).
The overlap of cancer cases on the map allowed researchers to understand that where a person lives and their social condition interfere with their access to diagnosis and their chances of surviving cancer in Campinas.
Clarification note: The study in question is limited to epidemiological analyses and did not directly investigate the causal determinants of the findings. Therefore, the interpretations presented are based on accumulated knowledge from the scientific literature in cancer epidemiology, which may not fully reflect the specificities of the local context of Campinas.
Authors of the study:
Dr. Andrea Paula Bruno von Zuben — Epidemiologist, information coordinator at Mário Gatti Municipal Hospital (Campinas, São Paulo), and associated researcher at CEPID CancerThera.
Dr. Maria do Carmo Ferreira — Postdoctoral researcher in the Research and Teaching Projects Program of the National Cancer Institute.
Dr. Marilisa Berti de Azevedo Barros — Full Professor of Epidemiology at FCM/Unicamp.
Ms. Juliana Nativo — Coordinator of the Population-Based Cancer Registry at the Health Surveillance Department.
Dr. M. Elvira P. Correa — Postdoctoral researcher in Executive Research Management at CEPID CancerThera, at Hemocentro/Unicamp.
Dr. Carmino Antônio de Souza — Full Professor of Hematology at FCM/Unicamp and principal investigator of CEPID CancerThera at Hemocentro/Unicamp.
Text: Romulo Santana Osthues